| HESITANCY TYPE | PATIENT MAY SAY OR ASK | POTENTIAL RESPONSE |
| Time restraints | “This is not a good time.” OR “I don’t have time today.“ | “I understand that you are busy. During this time, we want to continue providing thorough care for the best health and emotional outcomes for you and your family. This is one of many screenings to be completed as part of the your visit. If you cannot complete the screen at this time, can you please provide me with another date and time that works best for you and your family’s schedule.“ |
| Time restraints | “Can you call me back on [DATE and TIME].” | “Great, thank you. You are scheduled for [REPEAT DATE AND TIME]. If you have any questions, please feel free to contact us at __.” |
| Time restraints | “I can’t talk now and I don’t know when I will be available.“ | “Since you are unable to provide me with a date/time now, the office will follow-up with you soon. You will be asked to fill out this screening at routine visits. If you have any questions, please feel free to contact us at __.“ |
| General Skepticism | “Why are you asking?“ | “We screen patients and families during routine visits. Your answer helps us to assist you and your family with being healthy and happy.“ |
| General Skepticism | “No” OR “I’m not interested“ | “Can you please describe why you are not able to complete the screening(s) at this time? It is important for us to understand how we can make this experience easier for you and other patients. So many people have experienced these things, they are so common, that they actually created a screener for it. We ask EVERYBODY.“ *Clarify and acknowledge the individual concern* |
| Confidentiality | “Who will see my answers?” OR “Who wants to know?“ | “Your answers are kept confidential. Other healthcare providers or team members may know your answers only if it relates to your health and providing you care. If I am concerned about your safety, I may have to share your answers with others for your protection. If that is the case, though, I will let you know first and we can discuss. Are you in a private/safe space to speak?“ |
| Confidentiality | “I don’t want my family members/friends to find out.“ | “I understand your concern about discussing sensitive information. Your safety is our priority. If we do need to share information due to your safety being at risk, it will be with trusted professionals.“ |
| Confidentiality | “Why does all of the staff in the office need to be involved/why do they need to know my answers?“ | “As a team, we all are interested in providing you and your family with the best possible care, so it is important for us to communicate with one another to address the specific needs of you/your child.“ |
| If Pt/CG expresses NO despite above attempts | “I understand your reservations. I will allow your/your child’s provider to discuss the screening in further detail with you during your visit on [DATE AND TIME OF APPT].“ |
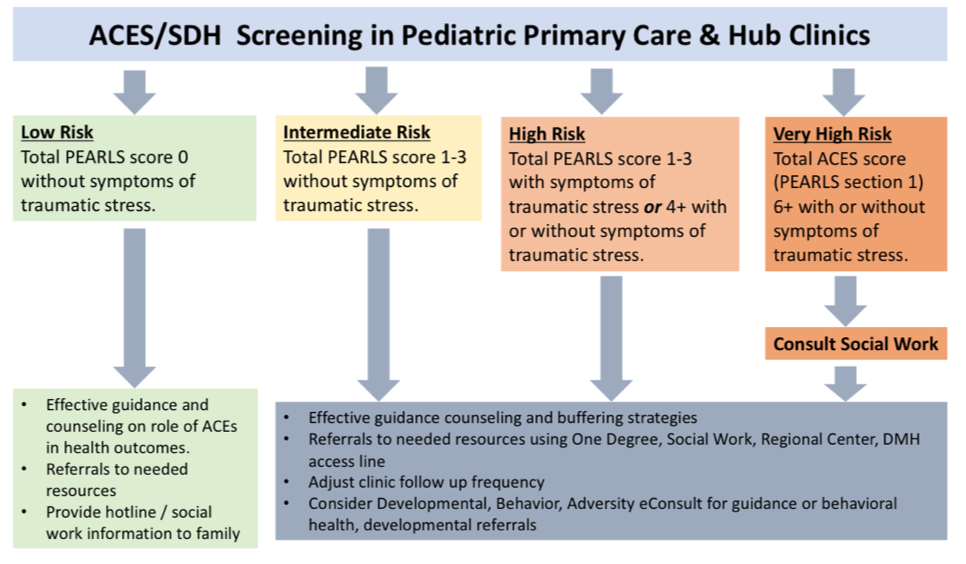
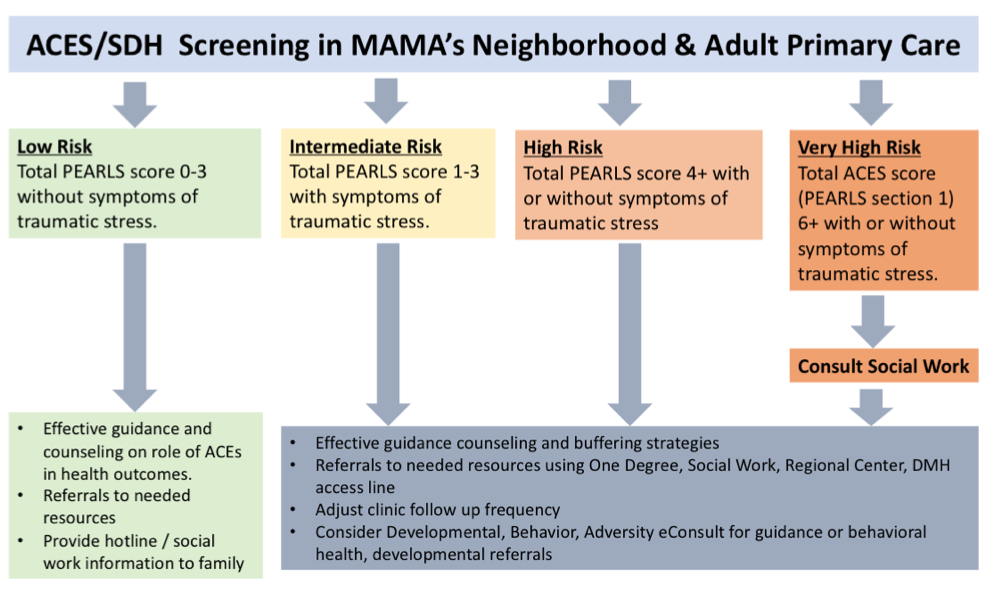
ACEs and SBDOH using the PEARLS tool
- Requirement – Screen patients at IHA, 9 month, 18 month, and 30 month visits, and yearly for ages 12 and older. Patients 18+ years should only be screened once.
- Introducing the questions – “The following questions are about potentially stressful experiences that can impact yours and your family’s health and well-being. Your answers can help your provider support you to prevent long-term health issues related to these stressful experiences.“
- Screening – ACEs/PEARLS/SBDOH in English or Spanish
- If the patient’s immediate health or safety is found to be at risk, please notify a provider immediately. The provider will determine next steps (ex: DCFS consult, Valley Coordinate Children’s Services referral/mobile response team, 9-1-1 or other)
- ORCHID Documentation – For all ages- enter results into ACES/PEARLS/SBDOH ad hoc form.
Ages and Stages Questionnaire (ASQ)
- Requirement – Screen patients at 9 months, 18 months, and 30 months and as needed from birth to 5 years.
- Introducing the questions – “The following questions come from the Ages and Stages Questionnaire. This will provide a quick check of your child’s development. It will show your child’s strengths and areas in which your child may need more help or practice. Your answers are kept confidential, and will help your provider know how better to support your child’s development.“
- Screening – ASQ Questionnaires
- ORCHID Documentation- Enter results in Pediatric Milestones ad hoc form. Scan questionnaire into ORCHID.
Generalized Anxiety Disorder (GAD) screen
- Requirement – Screen all 12 years and older yearly and as needed.
- Introducing the questions – “The following questions are used to check for signs or symptoms of anxiety. It helps your provider focus on your overall health and well-being.”
- Screening – Start with GAD2. If score 3 or more, ask the remaining 5 questions.
- If the patient’s immediate health or safety is found to be at risk, please notify a provider immediately. The provider will determine next steps (ex: DCFS consult, Valley Coordinate Children’s Services referral/mobile response team, 9-1-1 or other)
- ORCHID Documentation– For all ages – enter results into Anxiety Screening ad hoc form.
Modified Checklist for Autism in Toddlers- Revised (MCHAT-R)
- Requirement – Screen children at least once between 16 months and 30 months of age.
- Introducing the questions – “The following questions help determine the risk of autism in your child. You may have heard of autism. This is a developmental disorder that affects the ability to communicate and interact. It is not very common, but we screen for autism in young children because we know that early diagnosis can help support better treatments. I may ask you follow-up questions based on your first set of answers. We can’t diagnose your child with autism from this questionnaire, but can get a better idea if your child might need more testing to evaluate for autism.“
- Screening – Follow screening guidelines. If MCHAT-R score is 0-1, no further action needed. If MCHAT-R score is 3-7, administer the Follow-Up screen (MCHAT-R/F). If MCHAT score is 8-20, no further action needed; the provider will follow up.
- ORCHID Documentation- Enter result in Pediatric Milestones ad hoc form. Scan questionnaire into ORCHID.
Patient Health Questionnaire (PHQ)
- Requirement – Screen all mothers of infants at the baby’s newborn, 2 week, 1 month, 2 month, 4 month, and 6 month check-ups. Screen all 12 years and older yearly and as needed.
- Introducing the questions – “The following questions are used to check for signs or symptoms of depression. It helps your provider focus on your overall health and well-being.“
- Screening – Start with PHQ2. If score 3 or more, ask the remaining 7 questions.
- If the patient’s immediate health or safety is found to be at risk, please notify a provider immediately. The provider will determine next steps (ex: DCFS consult, Valley Coordinate Children’s Services referral/mobile response team, 9-1-1 or other)
- ORCHID Documentation – For all ages, enter results into Depression screening ad hoc form.
Staying Healthy Assessment
- Requirement – Must be completed for all IHAs; during the first scheduled preventive visit upon reaching a new SHA age group, and annually before reaching the next age group. Pediatric age groups are 0-6 months, 7-12 months, 1-2 years, 3-4 years, 5-8 years, 9-11 years, and 12-17 years. Adult age groups are 18-65 years and 65+ years.
- Introducing the questions – “The following questions come from the Staying Healthy Assessment. These help your provider understand your health so that they can help you adopt healthy behaviors.”
- Screening – SHA Questionnaires
- If the patient’s immediate health or safety is found to be at risk, please notify a provider immediately. The provider will determine next steps (ex: DCFS/APS consult, mental health referral/mobile response team, 9-1-1 or other)
- ORCHID Documentation– In pediatrics – document part of SHA in Pediatric Milestones ad hoc form. Otherwise, to be scanned into ORCHID.
LA County DHS: See job aids and screening tool charts.
AGES 0-18
ADULTS
| RISK LEVEL | POTENTIAL RESPONSE |
| Low Risk, no ACEs | “From what your telling me things are going well, that’s great to hear. We will provide you some material with health information for you and your family. A lot of our families find these materials to be useful.“ |
| Low Risk with history of some ACEs | “You mentioned that you have experienced some stresses. We want to assist you in any way that we can. We will provide you with some material with health information for you and your family. A lot of our families find these materials to be useful.“ |
| Intermediate Risk | “You mentioned you have experienced some stresses. We want to assist you in any way that we can. Would it be okay if we provide you with some material with health information for you and your family? A lot of our families find these materials to be useful.“ |
| High Risk | “When you answered this questionnaire you marked you have been through some difficult things. Many people in our community have been through a lot. Can you tell me what is causing you or your family stress, so that we can help you in the best way possible?“ |
| RISK LEVEL | POTENTIAL RESPONSE |
| Low Risk, no ACEs | “From what your telling me, things are going well, that’s great to hear. We will provide you some material with health information for you and your family, if you have not yet received it. A lot of our families find these materials to be useful.“ |
| Low Risk with history of some ACEs And Intermediate Risk And High Risk with <6 ACEs |
For adolescents and adults: “You mentioned you have experienced some stresses. Studies have shown that the more stressful events you experience as a child, the more likely you are to have long-term physical and mental health problems as an adult such as diabetes, high blood pressure, heart disease, depression, anxiety, etc. We have the opportunity to identify these risks so that we can help prevent or lower your health risks. The earlier we can address these stressors the faster the body can begin to work to adjust and heal.“ For providers: “You mentioned you have experienced some stresses. Studies have shown that the more stressful events you experience as a child, the more likely you are to have long-term physical health problems as an adult such as diabetes, high blood pressure, heart disease, etc. As the number of the stressful events your child is exposed to increases, your child’s risk for these health problems increases as well. We have the opportunity to identify these risks so that we can help prevent or lower the risk for health problems for your child. The earlier we can address these stressors the faster the body can begin to work to adjust and heal.“ |
| High Risk with 6+ ACEs | For adolescents and adults: “We understand that this questionnaire asks about experiences that may be difficult to discuss. The reason we ask you about these types of experiences is because research shows us that what we experience as kids and teenagers can affect us as adults. We want to know about your experiences in order to provide you with the best care possible that is specific to who you are and what you have been through. If you are not ready to talk now, that is okay, but I’d like to have someone from our medical team talk with you so that we can assist you in the best way possible.“ For providers: “We understand that this questionnaire asks about experiences that may be difficult to discuss. The reason we ask you about these types of experiences is because research shows us that what we experience as kids and teenagers can affect us as adults. We want to know about your child’s experiences in order to provide your child with the best treatment possible that is specific to who they are and what they have been through. If you are not ready to talk now, that is okay, but I’d like to have someone from our medical team talk with you so that we can assist you in the best way possible.“ |